Due to the sad demise of our beloved Dr.Shekhar Agarwal, his dedicated team of surgeons will be available for all your needs, please click on the below surgeon links to book an appointment with them
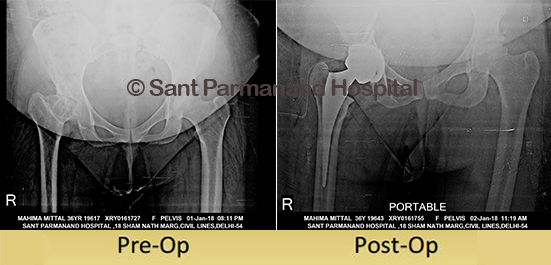
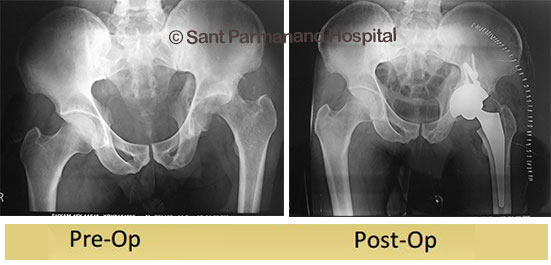
36 years old lady had developmental dysplasia of right hip. She had limp while walking since childhood and now had severe pain in walking. Her right leg was short by 3 cm. We did Uncemented Total Hip Replacement in which we create new artificial joint restoring the normal hip biomechanics . Total Hip Replacement in dysplastic hip is technical challenging surgery and very few centres across India are successfully performing this surgery. Now her legs are equal and her walk has improved. She is very happy with the result of surgery.
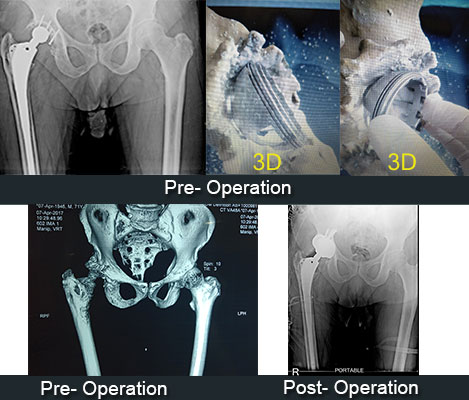
72 year old male whose primary THR was done in 1991 and revision THR for aseptic loosening was done in 2006 (both surgeries were performed elsewhere) presented to us with pain and instability.
Radiographs showed loose isoelastic acetabular cup and subluxed femoral head.
3D tissue printing images showed significant defect in the postero – superior wall of the acetabulum. 3D tissue printing is a new technology available at very few centers in country which allows precise preoperative planning of each patient.
Re-revision of the acetabular cup was done with an uncemented cup and around 40-50% of cup was found to be uncovered in the posterosuperior area for which a trabecular metal augment and autograft was used. Oxinium femoral head was implanted. Femoral stem was found to be well-fixed and was left in-situ. Patient was walking with walker support on second post operative day, he is relieved of pain and has regained limb length.
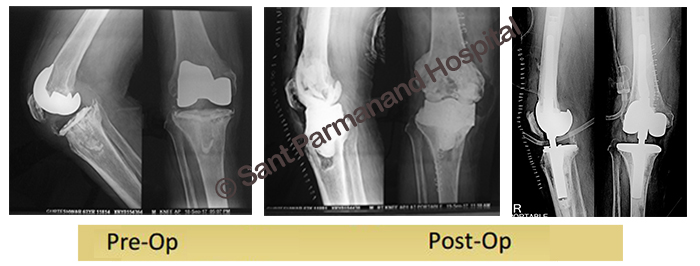
62 years gentleman presented to us with infected Right TKR which was performed 1 year ago elsewhere.
A 2 stage revision TKR was planned. In the first stage primary prosthesis was removed, thorough debridement was done and customized, mobile antibiotic cement spacer was placed in situ. Antibiotics were given for a total of 6 weeks till the infection was eradicated. 8 weeks later 2nd stage revision TKR done with RHK (Rotating Hinge Knee) and Stem Extender and Metallic Augment ( Distal and Posterior Femur Augments / Wedges).
Patient is comfortable and walking pain free with full weight bearing with no sign suggestive of recurrence of infection.
Revision TKR in the scenario of infection is challenging. At our center we have successfully managed many such cases.
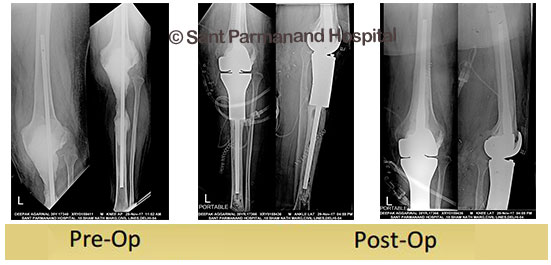
39 male gentleman presented to us with infection of left side knee. He had a history of proximal tibial tumour (osteosarcoma) which was treated by tumor resection and endoprosthesis 1 year back. He was in severe pain and was unable to bear weight on left side lower limb. Managing Infected Knee Replacement is a challenge and very few centres in India are managing these cases.
We at our centre follow 2 stage protocol for treatment of these case. In 1st stage the implants are removed and thorough debridement is done to clear of all the infection and antibiotic spacer are put for 3 months to clear the residual infection.
In 2nd Stage the antibiotic spacer are removed and revision Total Knee Implants are put. Patient can walk from 2nd post op day after this surgery. After surgery our patient is comfortable and walking independently. There are no signs of residual infection.
56 years old gentleman from Allahabad, sustained polytrauma 3 ½ months back with neglected fracture acetabulum left.
On examination hip was dislocated and femoral head was deformed. We planned uncemented Total Hip Replacement for the patient. THR in fracture acetabulum is challenging due to distorted anatomy and deficient bone stock. We reconstructed acetabulum with femoral head anatomy and used specialized continuum cup. Postoperatively patient is comfortable and walking with the help of walker.