Due to the sad demise of our beloved Dr.Shekhar Agarwal, his dedicated team of surgeons will be available for all your needs, please click on the below surgeon links to book an appointment with them
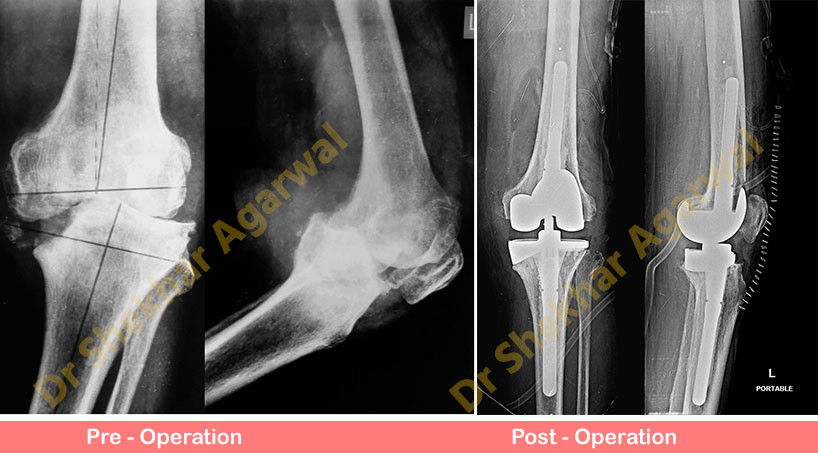
73 years old gentleman with advanced osteoarthritis knee came to us with complaints of pain and swelling since 6 months. He is unable to walk or stand. On Clinical examination he had severe varus deformity left knee and restricted range of motion was noticed. Preoperative X-Ray showed arthritic of knee joint with varus deformity and large medial tibial defect. These complex deformities need meticulous surgical planning in terms of bone cuts, defects management and ligaments balancing with revision constrained knee prosthesis.
The patient underwent total knee replacement surgery with constrained prosthesis and bone defect augmentation with wedge.
Post-operative X-Ray shows well balanced knee with constrained prosthesis (LCCK) with stemmed components and medial wedge (tibial side) to augment the defect. Now patient is comfortable and walking with support.
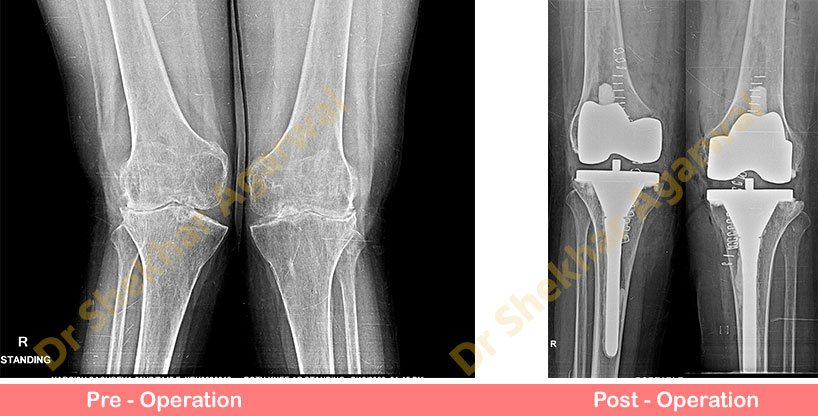
54 years old lady a case of rheumatoid arthritis came with pain and severe valgus deformities of both knees. She also had involvement of small joints of hand and feet.
Preoperative X-Rays showed bilateral valgus deformities with severe osteoporosis. These cases require meticulous preoperative planning for correct femoral and tibial component placement.
After appropriate ligament balance this case was managed with semiconstrained primary knee prosthesis with stem extension on tibial side to prevent implant subsidence because of osteoporosis.
Post op X-Rays show well aligned bilateral semiconstrained knee prosthesis with tibial stem extension. Patient is walking comfortably with walker.
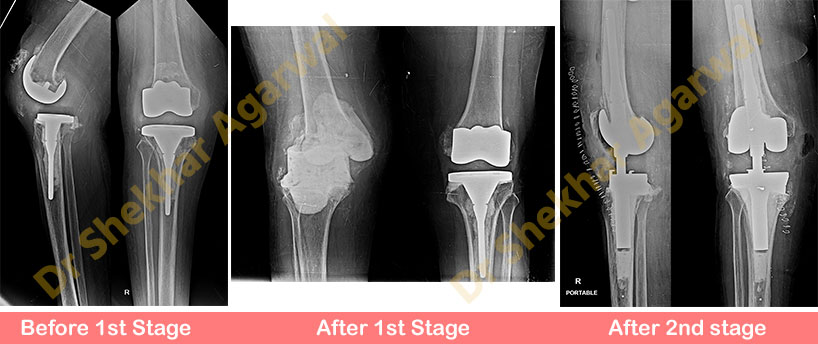
74 years old lady had undergone bilateral total knee replacement elsewhere in 2018. She presented with pain and discharging sinus over anterior aspect of right knee. All investigations pointed towards infection.
Two staged revision surgery was planned. In Aug 2020 (stage 1) removal of implant and thorough debridement was done and mobile antibiotic cement spacer was inserted.
In post op period, she was put on 6 weeks of antistaph antibiotics. After the infection settled 2nd stage surgery was done. The mobile antibiotic spacer was removed and rotating hinge knee prosthesis was inserted.
Post-operative X-Ray showed rotating hinge knee prosthesis. Now patient is comfortable and walking with support.
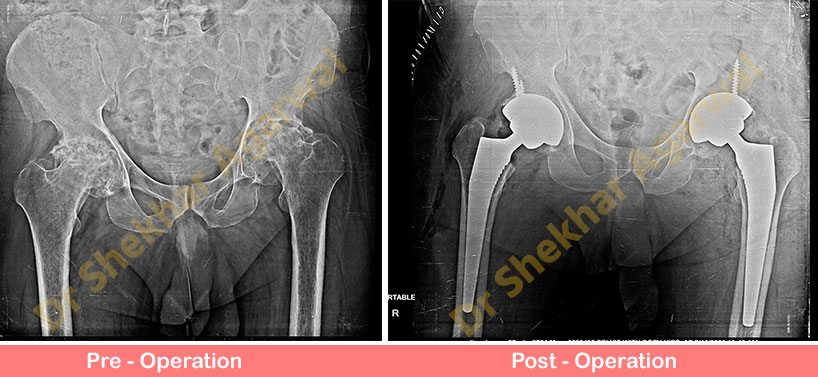
57 years old gentleman came with complaints of pain in both hips and difficulty in walking and doing daily routine activities for the past 5yrs. On Clinical examination all movements of hip were restricted and painful.
Preoperative xray showed arthritic (damaged) bilateral hip with avascular necrosis. We planned for bilateral hip replacement. These cases require meticulous preoperative and intraoperative planning to avoid limb length discrepancy with exact similar surgical procedure at both sides.
Postoperative X-Ray showed uncemeted hip replacement with equal limb length. Now patient is walking comfortably with walker.
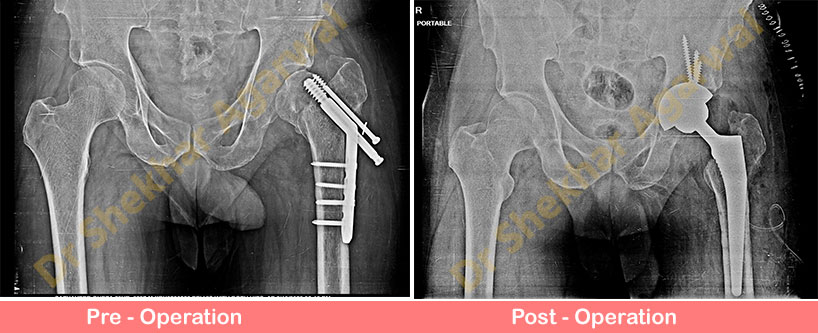
59 years old gentleman presented with complaints of pain in left hip and inability to bear full weight over left lower limb for the past 6 months. Patient had undergone fixation of the left hip fracture with dynamic hip screw and plate 1 year ago.
On Clinical examination there was shortening of 3 cm with local skin condition was normal. Infection markers were negative. Preoperative x-ray showed failed previous implant with avascular femoral head.
We removed the previous implant and converted this hip into Total Hip Replacement. Post operative x-ray shows uncemented THR. Now this patient is comfortable and the shortening of the leg has been corrected.